|
Description - CRPS RSD OVERVIEW
Reflex
Sympathetic Dystrophy Syndrome, RSDS, is now referred to as Complex
Regional Pain Syndrome, CRPS. CRPS is a progressive disease of the
Autonomic Nervous System whose pain is characterized as constant,
extremely intense, and out of proportion to the original injury. The
pain is typically accompanied by swelling, skin changes, sensitivity,
and can often be debilitating. It usually affects one or more of the
four limbs but can occur in any part of the body.
CRPS is ranked as the most painful form of chronic pain that exists today by the McGill Pain Index.
There are FOUR Main Symptoms/Criteria of CRPS:
There are a great many additional symptoms that can also occur over the course of the disease. Not all patients will have all symptoms and symptoms may change over time due to the stage the patient is in, the medications the patient is on, and/or the treatments the patient is receiving.
CRPS is ranked as the most painful form of chronic pain that exists today by the McGill Pain Index.
There are FOUR Main Symptoms/Criteria of CRPS:
There are a great many additional symptoms that can also occur over the course of the disease. Not all patients will have all symptoms and symptoms may change over time due to the stage the patient is in, the medications the patient is on, and/or the treatments the patient is receiving.
WHAT PARTS OF THE BODY ARE INVOLVED?
CRPS is a multi-symptom condition typically affecting one, two, or sometimes even all four extremities. It can also be in the face, shoulders, back, eyes, and other areas of the body as well. CRPS is an involvement of nerves, skin, muscles, blood vessels (causing constriction, spasms, and pain) as well as bones.
The Orthopod website describes this aspect very well:
"Sympathetic nerves are responsible for conducting sensation signals to the spinal cord from the body. They also regulate blood vessels and sweat glands. Sympathetic ganglia are collections of these nerves near the spinal cord. They contain approximately 20,000-30,000 nerve cell bodies. CRPS is felt to occur as the result of stimulation of sensory nerve fibers. Those regions of the body rich in nerve endings such as the fingers, hands, wrist, and ankles are most commonly affected. When a nerve is excited, its endings release chemicals. These chemicals cause vasodilation (opening of the blood vessels). This allows fluid to leak from the blood vessel into the surrounding tissue. The result is inflammation or swelling leading to more stimulation of the sensory nerve fibers. This lowers the pain threshold. This entire process is called neurogenic inflammation. This explains the swelling, redness, and warmth of the skin in the involved area initially. It also explains the increased sensitivity to pain. As the symptoms go untreated, the affected area can become cool, have hair loss, and have brittle or cracked nails. Muscle atrophy or shrinkage, loss of bone density (calcium), contracture, swelling, and limited range of motion in joints can also occur in the affected limb. These are in part caused by decreased blood supply to the affected tissues as the condition progresses." (Source: A Patient's Guide to Pain Management: Complex Regional Pain Syndrome)
DOES CRPS SPREAD?
It may spread from one part of the body to another regardless of where the original injury occurred; and CRPS can spread in up to 70% of the cases. However, in a small number of cases (8% or less) it can become Systemic or body-wide. (Source: Healing Soft Tissue Injuries: Muscles, Tendons, Fascia and More) CRPS usually spreads up/down the same limb, or to the opposite limb but in an increasing number of cases it spreads to other areas of the body.
WHO GETS CRPS?
ANYONE can get CRPS. There are millions of Women, Men, and Children across the country with this disease. It is estimated there are between 1.5 and 3 million victims in the United States alone. It affects women many more times than men; as many as 75% of victims are women. The majority of victims develop the disease in their 30's and 40's but it affects all age groups from birth to 103. Although in recent years more and more patients in their teens seem to be developing the disease. (2) The exact number of patients is unknown and estimates can vary widely.
CRPS OR RSDS? WHICH IS IT?
CRPS, RSDS, TYPE I or TYPE II? WHAT SHALL WE CALL IT TODAY? There have been so many questions about the name confusion surrounding RSD in the last couple of years. Is there a difference between RSDS and CRPS? What are the differences between RSDS and CRPS? One Dr tells me "You have RSD" while another says, "No, it is CRPS.", and a third tells me it is the same thing. Now I am totally confused. Which is the right term then? Why is a there a CRPS Type I and CRPS Type II; and what is the difference?
So gradually everyone, Doctors, the medical community, and patients as well, have gradually been switching over to the new language; CRPS Types I and II.
CRPS is a multi-symptom condition typically affecting one, two, or sometimes even all four extremities. It can also be in the face, shoulders, back, eyes, and other areas of the body as well. CRPS is an involvement of nerves, skin, muscles, blood vessels (causing constriction, spasms, and pain) as well as bones.
The Orthopod website describes this aspect very well:
"Sympathetic nerves are responsible for conducting sensation signals to the spinal cord from the body. They also regulate blood vessels and sweat glands. Sympathetic ganglia are collections of these nerves near the spinal cord. They contain approximately 20,000-30,000 nerve cell bodies. CRPS is felt to occur as the result of stimulation of sensory nerve fibers. Those regions of the body rich in nerve endings such as the fingers, hands, wrist, and ankles are most commonly affected. When a nerve is excited, its endings release chemicals. These chemicals cause vasodilation (opening of the blood vessels). This allows fluid to leak from the blood vessel into the surrounding tissue. The result is inflammation or swelling leading to more stimulation of the sensory nerve fibers. This lowers the pain threshold. This entire process is called neurogenic inflammation. This explains the swelling, redness, and warmth of the skin in the involved area initially. It also explains the increased sensitivity to pain. As the symptoms go untreated, the affected area can become cool, have hair loss, and have brittle or cracked nails. Muscle atrophy or shrinkage, loss of bone density (calcium), contracture, swelling, and limited range of motion in joints can also occur in the affected limb. These are in part caused by decreased blood supply to the affected tissues as the condition progresses." (Source: A Patient's Guide to Pain Management: Complex Regional Pain Syndrome)
DOES CRPS SPREAD?
It may spread from one part of the body to another regardless of where the original injury occurred; and CRPS can spread in up to 70% of the cases. However, in a small number of cases (8% or less) it can become Systemic or body-wide. (Source: Healing Soft Tissue Injuries: Muscles, Tendons, Fascia and More) CRPS usually spreads up/down the same limb, or to the opposite limb but in an increasing number of cases it spreads to other areas of the body.
WHO GETS CRPS?
ANYONE can get CRPS. There are millions of Women, Men, and Children across the country with this disease. It is estimated there are between 1.5 and 3 million victims in the United States alone. It affects women many more times than men; as many as 75% of victims are women. The majority of victims develop the disease in their 30's and 40's but it affects all age groups from birth to 103. Although in recent years more and more patients in their teens seem to be developing the disease. (2) The exact number of patients is unknown and estimates can vary widely.
CRPS OR RSDS? WHICH IS IT?
CRPS, RSDS, TYPE I or TYPE II? WHAT SHALL WE CALL IT TODAY? There have been so many questions about the name confusion surrounding RSD in the last couple of years. Is there a difference between RSDS and CRPS? What are the differences between RSDS and CRPS? One Dr tells me "You have RSD" while another says, "No, it is CRPS.", and a third tells me it is the same thing. Now I am totally confused. Which is the right term then? Why is a there a CRPS Type I and CRPS Type II; and what is the difference?
So gradually everyone, Doctors, the medical community, and patients as well, have gradually been switching over to the new language; CRPS Types I and II.
CRPS - WHAT DOES IT FEEL LIKE?
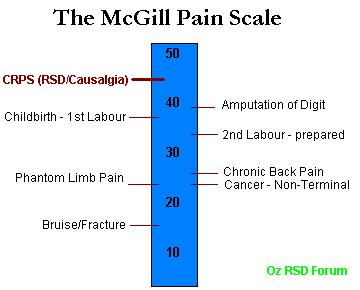
I was asked recently at my Doctors office by a visiting intern, "What does CRPS feel like?" This is a question I get asked quite often by the media as well. They want to know what the typical CRPS patient feels when they experience this pain. Every patient is asked this question now and again and you have to think of your answer by the way the person asked. How interested are they in your answer and how detailed an answer are they looking for? If they are asking what is CRPS pain is like in comparison to other diseases you give the McGILL Pain Index answer, "CRPS pain is ranked as the most painful form of chronic pain that exists today and is ranked on the McGill Pain Index at a whopping 42!" (look for "causalgia" on the chart). If they are asking as a friend and you don't want to scare them away you simply say "It is the most pain I have ever experienced, it hurts constantly."
After all, many patients have already lost a great many friends because of the disease and they don't want to lose more. If they are a loved one you try and protect them. You don't want them to know how bad it is. You don't ever want them to truly understand how much you suffer because you know how much they would then suffer as well. Many times your answer is simply, "I am fine. It is nothing I can't handle." Once in a great while you may let them know how truly horrible it is, after all, they see it in your eyes. But most of the time you try and shield them from the depth of your pain. If you have only had it for a year or two you aren't as skilled at hiding your pain, or controlling it, as someone who has had it for ten or more.
I think long-term chronic pain patients get so good at masking their pain, our pain, that when we have to reveal it, when we come upon circumstances where medical professionals need to see the actual level of pain we are in, it is difficult for us to convey the depth of the pain, to truly let down our guard, those walls we have built up, for fear of not being able to put them back up again. It can actually be difficult to completely let down those protective barriers to reveal exactly how much pain we are in and many times our Drs, especially new ones, don't realize just how bad our pain actually is.
So, having said that, what does CRPS pain actually feel like? Let me share with you what I shared with my Doctor recently and maybe it will help you understand our pain a little better. CRPS pain can be anywhere in the body where there are nerves. Most commonly in the four extremities but some people have it in other areas such as eyes, ears, back, face, etc. What does it feel like? Well, if you had it in your hand, imagine your hand was doused in gasoline, lit on fire, and then kept that way 24 hours a day, 7 days a week, and you knew it was never going to be put out. Now imagine it both hands, arms, legs, feet, eyes, ears,; well, you get the picture. I sometimes sit there and am amazed that no one else can see the flames shooting off of my body.
The second component to CRPS is what is called Allodynia. Allodynia is an extreme sensitivity to touch, sound, and/or vibration. Imagine that same hand now has the skin all burned off and is completely raw. Next, rub some salt on top of it and then rub some sandpaper on top of that! THAT is allodynia! Picture getting pretty vivid? Now, because of the allodynia, any normal touch will cause pain; your clothing, the gentle touch of a loved one, a sheet, rain, shower, razor, hairbrush, shoe, someone brushing by you in a crowded hallway, etc. In addition, sounds, especially loud or deep sounds and vibrations, will also cause pain; a school bell, thunder, loud music, crowds, singing, yelling, sirens, traffic, kids screaming, loud wind, even the sound in a typical movie theatre. This is what allodynia is all about. Imagine going through your daily life where everything that you touch, or that touches you, where most every noise around you from a passing car or plane to children playing, causes you pain. In addition to the enormous pain you are already experiencing from the CRPS itself. Imagine living with that pain and allodynia 24 hours a day, every day, for months, years, and longer. There are many other symptoms which you can read about in our CRPS SYMPTOMSsection but these are the two main ones that most patients talk about the most.
I hope this helps you understand what we deal with every day.
Peace, Keith Orsini
INCIDENCE OF CRPS
According to the National Institute of Neurological Disorders and Stroke (NINDS) and the National Institutes of Health (NIH) "it has been estimated that CRPS may present itself in 2-5% of individuals with peripheral nerve injury" ( See National Institutes of Health - NIH CRPS INCIDENCE or the NINDS website as well).
DOES CRPS GO INTO REMISSION? OR BURN ITSELF OUT?
These are two of the most commonly asked questions.
REMISSION AND CRPS
Will your CRPS go into remission? Unfortunately, not very likely but it depends on the age of the patient and the type of injury sustained. The incidence of remission is extremely low. It is highest for teens, especially if they are diagnosed within 1 to 12 months and treated aggressively. For adults, the need for quick diagnosis is even more urgent; within the first 3 to 6 months is imperative and that must be followed with aggresive therapy. The type of therapy depends on the type of CRPS you are diagnosed with. Newer treatments, especially the ketamine infusion in-hospital 5 day Awake technique, are proving successful in more than half of the patients treated and many are experiencing complete pain relief for up to 1, 2 years or more. As the study of CRPS continues and more is learned the hope is that more patients will be able to experience longer periods of pain relief. But again, the relief is temporary and not a cure.
IS IT CONSIDERED REMISSION IF I AM NOT IN PAIN BUT STILL TAKE PAIN MEDICATION?
This is a question we get asked quite often. Patients get their pain under control with the help of some of the wonderful physicans and therapists out there through the use of medications and physical therapy; usually a combination of aqua therapy and cardio, such as treadmill or stationary bike. The less pain they are in the more they can do physically, the better mood they are in emotionally, the better they sleep, sometimes leading to the need for even less pain medication; it is all a great healing cycle. For some, their pain goes away completely but they still need the medication to keep it away. Does this mean true remission then? The answer could be debated back and forth forever but the bottom line is, does it matter? If you have no pain and have improved your quality of life enjoy it! Take extra precautions, absolutely. Someone who has had CRPS once is more likely to have a recurrence than someone who has never had it, but don't let that thought rule your life.
WILL MY CRPS BURN ITSELF OUT IN A YEAR OR TWO?
No one is really sure how this Urban myth got started but it is amazing how many patients are told this by their Doctors still to this day with all the knowledge now available on this disease. The answer is no. Your CRPS will not burn itself out. Not in a year, not in two or three or more. (I sound like Dr Seuss!) What does that even mean? Ask your Doctor if they ever tell you that, to define what that phrase actually means, physiologically. Ask them to describe the process of CRPS burning out.
Does that mean you will have CRPS forever? Not everyone will, no. But there is simply no way to determine ahead of time how long yours will last. It could be a few years it could be many years. There just isn't enough empirical evidence collected to say one way or another. Much more research is needed into this disease. This is another reason why we need so desperately to raise awareness.
THE ORIGINS OF COMPLEX REGIONAL PAIN SYNDROME
CRPS has been documented since the Civil War under many different names. It was first studied by Dr. Weir Mitchell. In October of 1864 the first dent in the armor of CRPS was made. Weir Mitchell and his associates G.R. Moorheouse and W.W. Keen published a book called "Gunshot Wounds and Other Injuries of Nerves". We were fortunate to be able to procure a copy of this book. This book contained the account of the symptoms and signs of peripheral nerve injuries as they had observed them in Unionist soldiers at Turners Alne Hospital for Nervous Diseases in Philadelphia. Their description is so classic and vivid that it deserves an abbreviated quotation here.
"In our early experience of nerve wounds, we met with a small number of men were suffering from a pain which they described as ‘burning‘ or as ‘mustard red-hot‘ or as ‘red-hot file rasping the skin‘ ... The seat of burning pain is very various; but it never attacks the trunk, rarely the arm or thigh, and not often the forearm and leg. It's favored site is the foot or hand. In these parts it is to be found most often where the nutritive skin-changes are met with; ... Its intensity varies from the most trivial burning to a state of torture, which can hardly be credited, but which reacts on the whole economy, until the general health is seriously affected. The part itself is not alone subject to a deep burning sensation, but becomes exquisitely hyperesthectic, so that a touch or tap of the finger causes pain. Exposure to the air is avoided by the patient with a care which seems absurd, and most of the bad cases keep the hand constantly wet, finding relief in the moisture rather than the coolness of the application. As the pain increases, the general sympathy becomes more marked. The temper changes and grows irritable, and the face becomes anxious, and has a look of weariness and suffering. The sleep is restless, and the constitutional condition, reacting on the wounded limb, exasperates the hyperestic state so that the rattling of a newspaper, a breath of air, the step of another across the ward, the vibrations caused by a military band, or the shock of the feet in walking, gives rise to an increase of pain. Perhaps few persons who are not physicians can realize the influence which long continued and unendurable pain may have on both the body and mind. Under such torments the temper changes, the most amiable become irritable, the bravest soldier becomes a coward, and the strongest man is scarcely less nervous than the most hysterical girl."
Three years later, Mitchell first used the term Causalgia (from the Greek kausis-burning and algos-pain). It was right on the money then, and still is today. We must now teach Drs., Nurses, and others in the health care industry to diagnose it earlier and treat it faster and more aggressively.
McGill Pain Index
So many have asked us for a picture of the McGill Pain Index, so here it is. There are many versions out there. This one includes various types of childbirth pain as well. Causalgia is Latin for "burning pain". It was the first name coined for CRPS. As you can see, Causalgia is far and away the most painful form of Chronic Pain that exists! This is a good tool to use with your loved ones to help them compare our pain with other diseases and problems they can relate to. It also helps you to see that you are NOT exaggerating your pain one little bit! It is also a good graphic to use when fighting for Social Security Disability. The McGill Pain Index was first developed in 1971 as a way of gauging the quality of pain. It was developed at McGill University by Melzack and Torgerson. When creating this index they included such things as sensory qualities (skin color, temperature changes, pressure, sensitivity), affective qualities (tension, fear and autonomic properties), and evaluative issues that are help pinpointing the intensity of the pain. This Index is used by doctors and hospitals around the world and is considered a very valuable tool when looking at chronic pain It is considered to be a valid, reliable, consistent, and above all, useful instrument.
"Because pain is a private, personal experience, it is impossible for us to know precisely what someone else's pain feels like. No man can possibly know what it is like to have menstrual cramps or labour pain. Nor can a psychologically healthy person know what a psychotic patient is feeling when he says he has excruciating pain...There is a remarkable consistency in the choice of words by patients suffering the same or similar pain syndromes"
--Wall, P. D. And Melzack, R. (1994), Textbook of Pain, Churchhill Livingstone, New York, pp. 339-345.
I was asked recently at my Doctors office by a visiting intern, "What does CRPS feel like?" This is a question I get asked quite often by the media as well. They want to know what the typical CRPS patient feels when they experience this pain. Every patient is asked this question now and again and you have to think of your answer by the way the person asked. How interested are they in your answer and how detailed an answer are they looking for? If they are asking what is CRPS pain is like in comparison to other diseases you give the McGILL Pain Index answer, "CRPS pain is ranked as the most painful form of chronic pain that exists today and is ranked on the McGill Pain Index at a whopping 42!" (look for "causalgia" on the chart). If they are asking as a friend and you don't want to scare them away you simply say "It is the most pain I have ever experienced, it hurts constantly."
After all, many patients have already lost a great many friends because of the disease and they don't want to lose more. If they are a loved one you try and protect them. You don't want them to know how bad it is. You don't ever want them to truly understand how much you suffer because you know how much they would then suffer as well. Many times your answer is simply, "I am fine. It is nothing I can't handle." Once in a great while you may let them know how truly horrible it is, after all, they see it in your eyes. But most of the time you try and shield them from the depth of your pain. If you have only had it for a year or two you aren't as skilled at hiding your pain, or controlling it, as someone who has had it for ten or more.
I think long-term chronic pain patients get so good at masking their pain, our pain, that when we have to reveal it, when we come upon circumstances where medical professionals need to see the actual level of pain we are in, it is difficult for us to convey the depth of the pain, to truly let down our guard, those walls we have built up, for fear of not being able to put them back up again. It can actually be difficult to completely let down those protective barriers to reveal exactly how much pain we are in and many times our Drs, especially new ones, don't realize just how bad our pain actually is.
So, having said that, what does CRPS pain actually feel like? Let me share with you what I shared with my Doctor recently and maybe it will help you understand our pain a little better. CRPS pain can be anywhere in the body where there are nerves. Most commonly in the four extremities but some people have it in other areas such as eyes, ears, back, face, etc. What does it feel like? Well, if you had it in your hand, imagine your hand was doused in gasoline, lit on fire, and then kept that way 24 hours a day, 7 days a week, and you knew it was never going to be put out. Now imagine it both hands, arms, legs, feet, eyes, ears,; well, you get the picture. I sometimes sit there and am amazed that no one else can see the flames shooting off of my body.
The second component to CRPS is what is called Allodynia. Allodynia is an extreme sensitivity to touch, sound, and/or vibration. Imagine that same hand now has the skin all burned off and is completely raw. Next, rub some salt on top of it and then rub some sandpaper on top of that! THAT is allodynia! Picture getting pretty vivid? Now, because of the allodynia, any normal touch will cause pain; your clothing, the gentle touch of a loved one, a sheet, rain, shower, razor, hairbrush, shoe, someone brushing by you in a crowded hallway, etc. In addition, sounds, especially loud or deep sounds and vibrations, will also cause pain; a school bell, thunder, loud music, crowds, singing, yelling, sirens, traffic, kids screaming, loud wind, even the sound in a typical movie theatre. This is what allodynia is all about. Imagine going through your daily life where everything that you touch, or that touches you, where most every noise around you from a passing car or plane to children playing, causes you pain. In addition to the enormous pain you are already experiencing from the CRPS itself. Imagine living with that pain and allodynia 24 hours a day, every day, for months, years, and longer. There are many other symptoms which you can read about in our CRPS SYMPTOMSsection but these are the two main ones that most patients talk about the most.
I hope this helps you understand what we deal with every day.
Peace, Keith Orsini
INCIDENCE OF CRPS
According to the National Institute of Neurological Disorders and Stroke (NINDS) and the National Institutes of Health (NIH) "it has been estimated that CRPS may present itself in 2-5% of individuals with peripheral nerve injury" ( See National Institutes of Health - NIH CRPS INCIDENCE or the NINDS website as well).
DOES CRPS GO INTO REMISSION? OR BURN ITSELF OUT?
These are two of the most commonly asked questions.
REMISSION AND CRPS
Will your CRPS go into remission? Unfortunately, not very likely but it depends on the age of the patient and the type of injury sustained. The incidence of remission is extremely low. It is highest for teens, especially if they are diagnosed within 1 to 12 months and treated aggressively. For adults, the need for quick diagnosis is even more urgent; within the first 3 to 6 months is imperative and that must be followed with aggresive therapy. The type of therapy depends on the type of CRPS you are diagnosed with. Newer treatments, especially the ketamine infusion in-hospital 5 day Awake technique, are proving successful in more than half of the patients treated and many are experiencing complete pain relief for up to 1, 2 years or more. As the study of CRPS continues and more is learned the hope is that more patients will be able to experience longer periods of pain relief. But again, the relief is temporary and not a cure.
IS IT CONSIDERED REMISSION IF I AM NOT IN PAIN BUT STILL TAKE PAIN MEDICATION?
This is a question we get asked quite often. Patients get their pain under control with the help of some of the wonderful physicans and therapists out there through the use of medications and physical therapy; usually a combination of aqua therapy and cardio, such as treadmill or stationary bike. The less pain they are in the more they can do physically, the better mood they are in emotionally, the better they sleep, sometimes leading to the need for even less pain medication; it is all a great healing cycle. For some, their pain goes away completely but they still need the medication to keep it away. Does this mean true remission then? The answer could be debated back and forth forever but the bottom line is, does it matter? If you have no pain and have improved your quality of life enjoy it! Take extra precautions, absolutely. Someone who has had CRPS once is more likely to have a recurrence than someone who has never had it, but don't let that thought rule your life.
WILL MY CRPS BURN ITSELF OUT IN A YEAR OR TWO?
No one is really sure how this Urban myth got started but it is amazing how many patients are told this by their Doctors still to this day with all the knowledge now available on this disease. The answer is no. Your CRPS will not burn itself out. Not in a year, not in two or three or more. (I sound like Dr Seuss!) What does that even mean? Ask your Doctor if they ever tell you that, to define what that phrase actually means, physiologically. Ask them to describe the process of CRPS burning out.
Does that mean you will have CRPS forever? Not everyone will, no. But there is simply no way to determine ahead of time how long yours will last. It could be a few years it could be many years. There just isn't enough empirical evidence collected to say one way or another. Much more research is needed into this disease. This is another reason why we need so desperately to raise awareness.
THE ORIGINS OF COMPLEX REGIONAL PAIN SYNDROME
CRPS has been documented since the Civil War under many different names. It was first studied by Dr. Weir Mitchell. In October of 1864 the first dent in the armor of CRPS was made. Weir Mitchell and his associates G.R. Moorheouse and W.W. Keen published a book called "Gunshot Wounds and Other Injuries of Nerves". We were fortunate to be able to procure a copy of this book. This book contained the account of the symptoms and signs of peripheral nerve injuries as they had observed them in Unionist soldiers at Turners Alne Hospital for Nervous Diseases in Philadelphia. Their description is so classic and vivid that it deserves an abbreviated quotation here.
"In our early experience of nerve wounds, we met with a small number of men were suffering from a pain which they described as ‘burning‘ or as ‘mustard red-hot‘ or as ‘red-hot file rasping the skin‘ ... The seat of burning pain is very various; but it never attacks the trunk, rarely the arm or thigh, and not often the forearm and leg. It's favored site is the foot or hand. In these parts it is to be found most often where the nutritive skin-changes are met with; ... Its intensity varies from the most trivial burning to a state of torture, which can hardly be credited, but which reacts on the whole economy, until the general health is seriously affected. The part itself is not alone subject to a deep burning sensation, but becomes exquisitely hyperesthectic, so that a touch or tap of the finger causes pain. Exposure to the air is avoided by the patient with a care which seems absurd, and most of the bad cases keep the hand constantly wet, finding relief in the moisture rather than the coolness of the application. As the pain increases, the general sympathy becomes more marked. The temper changes and grows irritable, and the face becomes anxious, and has a look of weariness and suffering. The sleep is restless, and the constitutional condition, reacting on the wounded limb, exasperates the hyperestic state so that the rattling of a newspaper, a breath of air, the step of another across the ward, the vibrations caused by a military band, or the shock of the feet in walking, gives rise to an increase of pain. Perhaps few persons who are not physicians can realize the influence which long continued and unendurable pain may have on both the body and mind. Under such torments the temper changes, the most amiable become irritable, the bravest soldier becomes a coward, and the strongest man is scarcely less nervous than the most hysterical girl."
Three years later, Mitchell first used the term Causalgia (from the Greek kausis-burning and algos-pain). It was right on the money then, and still is today. We must now teach Drs., Nurses, and others in the health care industry to diagnose it earlier and treat it faster and more aggressively.
McGill Pain Index
So many have asked us for a picture of the McGill Pain Index, so here it is. There are many versions out there. This one includes various types of childbirth pain as well. Causalgia is Latin for "burning pain". It was the first name coined for CRPS. As you can see, Causalgia is far and away the most painful form of Chronic Pain that exists! This is a good tool to use with your loved ones to help them compare our pain with other diseases and problems they can relate to. It also helps you to see that you are NOT exaggerating your pain one little bit! It is also a good graphic to use when fighting for Social Security Disability. The McGill Pain Index was first developed in 1971 as a way of gauging the quality of pain. It was developed at McGill University by Melzack and Torgerson. When creating this index they included such things as sensory qualities (skin color, temperature changes, pressure, sensitivity), affective qualities (tension, fear and autonomic properties), and evaluative issues that are help pinpointing the intensity of the pain. This Index is used by doctors and hospitals around the world and is considered a very valuable tool when looking at chronic pain It is considered to be a valid, reliable, consistent, and above all, useful instrument.
"Because pain is a private, personal experience, it is impossible for us to know precisely what someone else's pain feels like. No man can possibly know what it is like to have menstrual cramps or labour pain. Nor can a psychologically healthy person know what a psychotic patient is feeling when he says he has excruciating pain...There is a remarkable consistency in the choice of words by patients suffering the same or similar pain syndromes"
--Wall, P. D. And Melzack, R. (1994), Textbook of Pain, Churchhill Livingstone, New York, pp. 339-345.
NERVOUS SYSTEM
Here is a full body diagram showing the nervous system (click on it to enlarge)
Here is a full body diagram showing the nervous system (click on it to enlarge)

NERVOUS SYSTEM CHART
HERE IS AN CHART OF THE NERVOUS SYSTEM (click on it to enlarge)
HERE IS AN CHART OF THE NERVOUS SYSTEM (click on it to enlarge)

....AND BASICALLY, THE NERVES IN THE SYMPATHETIC
NERVOUS SYSTEM ARE AT WAR, AND ARE CONSTANTLY FIRING....AROUND THE
CLOCK, 24 HOURS A DAY/7 DAYS A WEEK, 365 DAYS A YEAR.
No comments:
Post a Comment